


A periodical journal "Bulletin of maternal and child care" dedicated to fundamental and applied scientific research in the field of clinical medicine, biomedical sciences, and preventive medicine. The journal includes sections devoted to the problems of obstetrics, gynecology, reproduction, fetal surgery, endocrinology, pediatrics, neonatology, anesthesiology and resuscitation, immunology and microbiology, pathomorphology and cytodiagnostics, medical and laboratory genetics
The magazine is published four times a year.
Particular attention is paid to regional features of the diagnosis and treatment of diseases, as well as the specifics of the organization of healthcare in the Ural Federal District.
The journal is open for cooperation with Russian specialists and specialists from near and far abroad. The editors accept articles in English and Russian. The best, in the opinion of the editorial board, Russian-language articles are translated into English. Articles received by the editor in English are published accompanied by Russian-language metadata.
Current issue
EDITORIAL

Early pediatric neurorehabilitation is a healthcare priority because it leverages the high neuroplasticity of the brain during the first years of life and helps reduce the risk of persistent motor, cognitive, and behavioral impairments. This paper summarizes the biological determinants of the effectiveness of early interventions (synaptogenesis, myelination, critical periods) and highlights that, in the absence of timely support, neuroplasticity may consolidate ineffcient compensatory strategies, increasing the likelihood of secondary complications. The “first 1000 days” concept is discussed as a clinically meaningful window of opportunity, emphasizing the need to initiate rehabilitation as early as possible after medical stabilization, ensure regular practice, and actively involve the family. We systematize the main groups of children who should be referred to early neurorehabilitation: infants at perinatal risk of central nervous system injury, preterm infants, children with neurodevelopmental disorders, congenital and genetic/metabolic conditions affecting development, sequelae of acquired brain injury, and sensory impairments, as well as children exposed to combined biological and psychosocial risk factors. The paper underscores that effective early intervention requires a multidisciplinary model, continuity of care pathways, and a focus on functional goals.
REVIEWS
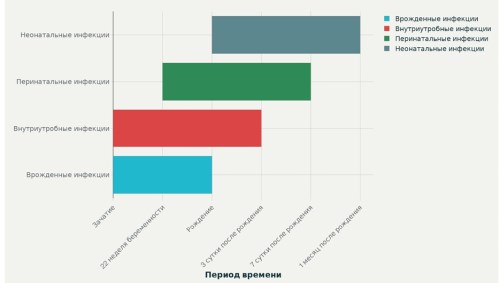
The publication provides clinical and diagnostic features of congenital, intrauterine, perinatal and postnatal infections in newborns based on a review of current clinical guidelines. There are common patterns and similar clinical manifestations for all of these infections, but there are significant differences. Attention is paid to the importance of isolating the “TORCH” syndrome in newborn children in order to carry out subsequent diagnosis of the etiology of infection. Additional information about intraamniotic infection is provided. Methods of laboratory diagnosis of infection are presented. Direct methods are described: microscopy, polymerase chain reaction, bacteriological (culture) method. Among the indirect diagnostic methods, information is provided on enzyme immunoassay, determination of immunoglobulins M and G. Attention is paid to the importance of studying the avidity of immunoglobulins G. The detection of low-avidity antibodies confirms acute infection. The presence of highly specific antibodies makes it possible to establish a history of infection. The advantages and disadvantages of direct and indirect methods of diagnosing infection in children are described. First of all, patients should be examined for those infections for which etiological and pathogenetic treatment has been developed. The main goal of therapy is to reduce the replication of the infectious agent in order to prevent damage to cells and tissues. The criterion for the effectiveness of therapy is considered to be the positive dynamics of the child’s condition, as well as the negative results of the polymerase chain reaction.
The deterioration of maternal health and the increasing percentage of women with pregnancy complications lead to disrupted lactation and, consequently, a decrease in breastfeeding rates in this group of infants during the first year of life. Research on antenatal breast milk expression is relevant due to the need to evaluate its effectiveness in correcting hypoglycemia in newborns of mothers with gestational diabetes, as well as ensuring safety for mothers.
The purpose of the study: Analysis of foreign experience in the implementation of prenatal pumping of breast milk, in order to prevent hypogalactia and hypoglycemia in children from mothers with gestational diabetes mellitus.
Materials and methods. The review includes published data for the last 16 years. The literature was searched in the Medline and PubMed databases.
Results. Currently, there are no unified approaches to prenatal pumping in world practice. The safety of antenatal pumping in the analyzed literature has been confirmed at 34 to 37 weeks of gestation, while the safety at an earlier stage remains insuffciently investigated. As a preventive measure of hypogalactia, prenatal pumping of breast milk promotes the early establishment of lactation, but does not demonstrate a statistically significant relationship with the frequency of hypoglycemia and the need for intensive therapy in newborns with diabetic fetopathy.
Conclusion. An analysis of the literature data has shown that prenatal pumping of breast milk has an ambiguous prognosis in the prevention of hypoglycemia in newborns with diabetic fetopathy. In turn, prenatal pumping of breast milk has a beneficial effect on the establishment of lactation, reduces the frequency of use of breast milk substitutes.
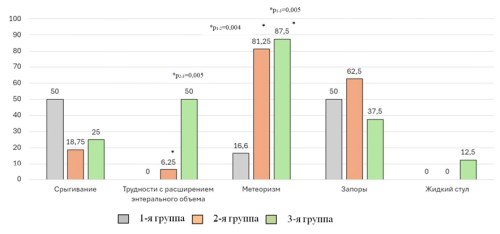
Rumination is repetitive, effortless regurgitation (regurgitation) of food on time or shortly after eating, followed by chewing, swallowing, or spitting out. Low awareness among pediatricians leads to underdiagnosis of rumination in children and ineffective treatment. Rumination occurs mainly in infants aged 3 to 12 months. In diagnosis, careful collection of medical history and assessment of the clinical picture is of the greatest importance. Most often, parents complain of vomiting and regurgitation in the child. It is optimal to make a video recording of regurgitation episodes for subsequent assessment. Rumination according to Roman criteria IV refers to functional disorders of the gastrointestinal tract. A child with rumination should have no symptoms of organic pathology. Children should be excluded from congenital malformations, surgical pathology, infectious and metabolic diseases. The diagnosis requires laboratory and instrumental examination, and consultations with a surgeon, gastroenterologist, and psychologist are necessary. Timely diagnosis and treatment of rumination plays a key role in preventing complications, ensuring normal growth and development of the child. It is necessary to train parents in child care skills and feeding rules. In infants with rumination, the use of proton pump inhibitors, prokinetics, and antacids is not recommended in routine practice. Behavioral therapy, diaphragmatic breathing training, and family psychosocial support are of the most important importance in the treatment of rumination.
ORIGINAL ARTICLES
Introduction. Hemolytic disease of the newborn (HDN), despite significant advances achieved in its prevention and treatment, continues to contribute substantially to the structure of perinatal pathology, being a cause of severe complications.
Objective. To assess the necessity for a differentiated approach to the therapy of hemolytic disease of the newborn depending on its severity and the number of intrauterine hemotransfusions in the setting of a specialized intensive care unit.
Materials and Methods. A prospective cohort study was conducted, including 61 children with an established diagnosis of rhesus immunization of the fetus and newborn (ICD-10, P55.0), who received treatment in the intensive care unit and the neonatal pathology department. Group 1 consisted of 29 children without intrauterine correction of HDN. Group 2 consisted of 19 children who required 1–2 intrauterine intravascular blood transfusions for severe fetal hemolytic disease. Group 3 included 13 children who underwent 3 or more intrauterine intravascular blood transfusions. The study analyzed treatment strategies and the duration of children’s hospital stay depending on the presence and number of intrauterine interventions.
Results. The study revealed significant differences in the course of hemolytic disease of the newborn (HDN) depending on the presence and number of performed intrauterine blood transfusions (IUT). Newborns who underwent multiple intrauterine blood transfusions (IUT) demonstrated the most aggressive disease course, manifested by a significantly higher need for exchange blood transfusion (ET) and hemotransfusions at the start of treatment. On the other hand, it was this category of patients that showed more favorable dynamics regarding hyperbilirubinemia. In newborns who did not receive intrauterine correction of HDN, the need for ET was identified in approximately one-third of cases. However, it should be noted that in a larger number of cases, such children require repeated ETs. This group of children showed the lowest number of hemotransfusions, indicating a predominance of the icteric form of HDN with a less pronounced anemic component. The group of children who underwent 1-2 intrauterine blood transfusions occupied an intermediate position, combining clinical characteristics of both the first and third groups. The rate of requiring exchange blood transfusion (ET) in these patients was 36.8%, which is statistically comparable to the group without intrauterine interventions. At the same time, the need for hemotransfusions reached 42%, significantly exceeding the rate in the first group (17.2%) and approaching the values of the third group (38.4%).
Conclusion. The identified features of the pathogenesis and clinical course of HDN depending on the number of IUTs underscore the necessity of a differentiated approach to managing such patients, taking into account both the severity of the antenatal period and the specifics of postnatal adaptation.
Introduction. Severe birth asphyxia, as one of the main causes of perinatal morbidity and mortality, presents a serious problem in neonatology.
Study Objective: To identify the characteristics of the early neonatal period and its outcome in full-term newborns with severe birth asphyxia.
Materials and Methods. A prospective single-center study was conducted. The main group consisted of 30 newborns who experienced severe birth asphyxia, and the control group for comparison of blood gases and acid-base balance comprised 60 newborns without asphyxia. Statistical processing of the results was carried out using the “Microsoft Excel 2016” application software package. The following were calculated: mean value (M), Standard deviation (SD), frequencies (%), and Student’s t-test. The critical significance level for testing statistical hypotheses was taken as 0.05.
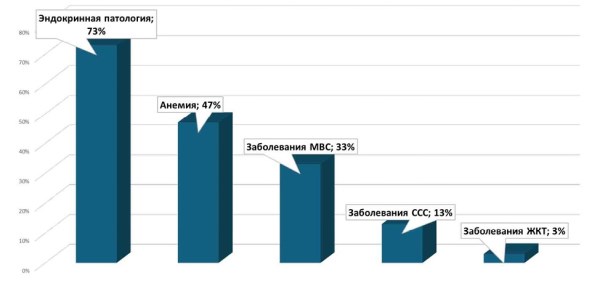
Results. Maternal medical history and the course of the current pregnancy were analyzed. Predominantly endocrine pathology was identified, including gestational diabetes mellitus in 95% of cases and obesity of varying severity. Delivery was operative in 53% of cases. In 57% of cases, complications included the development of fetal distress. The condition of newborns at birth reflected severe hypoxia: average Apgar scores were 2.43±0.77 at one minute, 4.76±1.22 at five minutes, and 6.2±1.22 at ten minutes. Respiratory support was required for all patients: in the delivery room, invasive mechanical ventilation (MV) was used in 73%, and continuous positive airway pressure (CPAP) in 37%. This was followed by transfer to the Neonatal Intensive Care Unit (NICU), where ventilation duration reached 20 days in severe cases. Passive hypothermia was initiated in 70% of newborns, and therapeutic hypothermia in 33%, which aligns with current neuroprotection protocols and emphasizes the need for early intervention to minimize neurological deficits. Neurosonography revealed cerebral ischemia in 90% of infants, with cerebral edema in 47% and periventricular lesions in 60%, illustrating a direct link between asphyxia and cerebral complications and multi-organ dysfunction.
Conclusion. In the vast majority of newborns, the early neonatal period concluded with the development of cerebral ischemia, predominantly of moderate severity (grade II), with periventricular brain injury detected in a significant number of cases. Further study and analysis of newborns who experienced severe birth asphyxia are necessary to identify predictors of adverse neurological outcomes.
Introduction: one of the basic indicators of the effectiveness of rehabilitation measures in children with neurological disorders is the psychological state of their parents, but it remains insuffciently studied in dozens of neurorehabilitation programs.
Study Objective: to conduct a comprehensive psychodiagnostic analysis of anxiety, nosognostic patterns, and parenting competencies in parents of children undergoing neurorehabilitation.
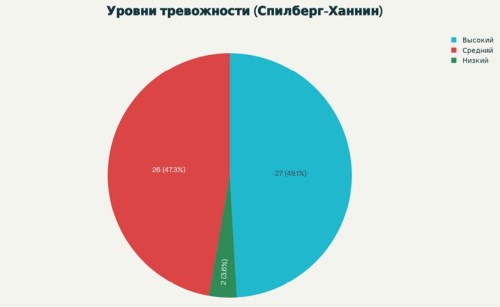
Materials and Methods. The study involved 59 mothers with children aged three months to six years. Standardized, validated, and psychometric instruments were used: Anxiety Scale, the Method for Assessing Attitudes Toward a Child’s Illness, and the Mindful Parenting Test. Additional sociopsychological characteristics were also examined: the child’s disability, the number of children in the family, region of residence, and offcial marital status. The statistical analysis included descriptive statistics and a correlation analysis of the relationships between sociodemographic and psychological indicators.
Results. 42% of families were raising children with disabilities, 33% were large families, and 28% lived in small towns and villages in the region. 76% of mothers were offcially married. The proportion of mothers without the above-mentioned characteristics was 16%. Hyperanxiety was identified in 49% of mothers, nosognostic disorders in 63%, and impaired parenting skills in 23%. The predominant pathological patterns were unruly behavior 40% and poor parenting skills 10%.
Conclusion. Parents of children requiring neurorehabilitation demonstrate a high prevalence of psychoemotional disorders and dysfunctional coping strategies, which justifies the need to include psychological support in rehabilitation protocols.
Introduction. Modern molecular and genetic studies refute the previous concept of the sterility of the intrauterine environment: it has been established that the fetal gastrointestinal tract already contains microorganisms, including Klebsiella pneumonia (KP), whose colonization is determined by a complex of perinatal factors (gestational age, type of feeding, stay in the intensive care unit, and antibiotic therapy). The outcome of colonization of the intestines of premature infants — from asymptomatic carriage to full-blown infection — is determined by the state of local mucosal protection, the immunological reactivity of the child, and the virulent properties of Klebsiella pneumoniae. The presence of genetically determined virulence factors in KP (genes fim, kfu, uge) and their potential impact on the course of the neonatal period justify the relevance of this study.
Study Objective. To study the key aspects of neonatal adaptation in premature newborns of gestational age 32–36 weeks and 6 days, whose intestines are colonized by Klebsiella pneumoniae with uge, fim, and kfu genes.
Materials and Methods. A survey was conducted on 30 newborns with a gestational age of 32–36 weeks and 6 days, whose intestines were colonized with Klebsiella pneumoniae (KP). Depending on the genovariant of the strains, the children were divided into three groups: Group 1 included premature infants colonized with KP uge (n=6), Group 2 included uge+fim (n=16), and Group 3 included kfu+uge+fim (n=8). A comprehensive assessment of clinical, laboratory, instrumental, and microbiological indicators was conducted in premature infants. Detection of uge, fim, and kfu genes was performed using real-time polymerase chain reaction (PCR).
Results. The article presents data on the course of the neonatal period in 32–36 weeks 6 days of GA children with CR with a different set of genes. It was shown that anthropometric data, the Apgar score, in all groups were comparable. Premature infants with kfu+uge+fim genes had the lowest levels of hemoglobin (113.37±14.82 g/l) and hematocrit (33.73±4.56%) on the 10th–14th day of life (p<0.001), the maximum duration of respiratory support (2.06±1.24 days; p=0.012) and antibacterial therapy (19.0±5.60 days; p=0.005), as well as deterioration with transfer to the ICU in 37.5% of cases. Children with the uge+fim genotype were more likely to have perinatal infections (81.25%; p<0.017) and retained colonization with K. pneumoniae at discharge (100%; p=0.002).
Conclusion. Since premature infants colonized with K. pneumoniae with uge+fim and kfu+uge genotypes remain bacteriologically positive by the time of discharge, the risk of Klebsiella infection persists due to immune immaturity, necessitating their follow-up.
MISCELLANEOUS
Introduction. Endometriomas are one of the most common gynecological diseases. Surgical removal of endometriomas is considered the standard treatment for large endometriomas and/or those associated with pain. However, despite the clinical effectiveness of endometrioma removal, this approach is associated with a number of reproductive risks.
Objective: to compare the effect of two intraoperative hemostasis methods – autologous platelet-rich fibrin glue versus standard bipolar coagulation – on ovarian function preservation after laparoscopic cystectomy of ovarian endometriomas.
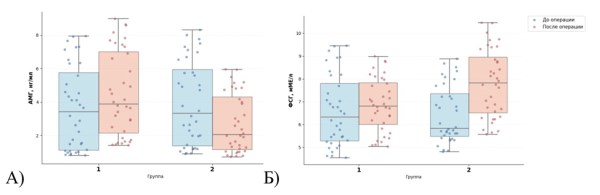
Materials and Methods: A prospective comparative cohort study was conducted involving 72 reproductive-aged women with ovarian endometriomas. Patients were allocated into two groups of 36 each. All patients underwent laparoscopic cystectomy. In Group 1, hemostasis was achieved using autologous platelet-rich fibrin glue; in Group 2, bipolar coagulation was applied. Ovarian reserve was assessed before and 6 months after surgery by measuring serum AMH, FSH, and CA-125 levels; ovarian volume, antral follicle count (AFC), and ovarian artery resistance index (RI) were evaluated by transvaginal ultrasound.
Results: Baseline demographic, hormonal, and ultrasound characteristics were comparable between groups. At 6 months postoperatively, the fibrin glue group showed significantly higher AMH levels compared to the coagulation group: 3.85 (1.89–7.17) vs. 2.1 (1.1–4.3) ng/mL, p=0.03. FSH levels significantly increased in Group 2 (p=0.03) but remained stable in Group 1. AFC in the operated ovary increased in the fibrin glue group (p=0.03) and did not change in the coagulation group. RI significantly decreased in both groups (p<0.01). Postoperative CA-125 levels were significantly lower in Group 1 (p=0.02).
Conclusion: The use of autologous platelet-rich fibrin glue for hemostasis during laparoscopic cystectomy of ovarian endometriomas provides significantly better preservation of ovarian function compared to bipolar coagulation. This technique may be recommended as a priority approach in patients desiring fertility preservation.

Introduction. Pelvic organ prolapse remains one of the most significant challenges in modern gynecology, profoundly affecting patients’ quality of life. Selecting a surgical strategy for young women is particularly complex due to their reproductive plans and the limitations on using synthetic meshes because of the risk of mesh-associated complications. Meanwhile, native tissue repair, while remaining the basic surgical approach, is associated with a significant risk of recurrence, especially in patients with underlying connective tissue incompetence. In this context, the search for biologically oriented, organ-preserving surgical techniques is highly relevant, aiming not only at mechanical correction but also at restoring the quality of the patient’s own pelvic floor tissues.
Objective. To present a clinical case of surgical treatment for recurrent stage III pelvic organ prolapse (POP-Q classification) in a woman of reproductive age, using native tissue repair combined with subfascial injection of micro-fragmented adipose tissue.
Materials and Methods. We performed treatment and clinical follow-up on a woman of reproductive age diagnosed with recurrent stage III pelvic organ prolapse (POP-Q classification), primarily involving the anterior compartment. The patient underwent organ-preserving surgery involving native tissue repair of the anterior vaginal wall combined with subfascial injection of micro-fragmented adipose tissue.
Results. Follow-up examinations at 1, 3, 6, and 12 months demonstrated restoration of normal pelvic anatomy: the position of the anterior vaginal wall corresponded to stage 0 prolapse according to the POP-Q system. No clinical or instrumental signs of cystocele recurrence were detected. The patient reported a significant improvement in quality of life, resolution of the sensation of vaginal bulging, absence of voiding symptoms, and restoration of sexual function.
Conclusion. The combined treatment method for recurrent pelvic organ prolapse — native tissue repair with subfascial injection of micro-fragmented adipose tissue — demonstrated clinical effcacy and safety in this reproductive-age patient. The approach restored anatomical support of the anterior compartment with no signs of recurrence during the 12-month follow-up, alleviated symptoms, and improved quality of life.












